
Health
What is a Dangerous Psa Level After Prostate Removal
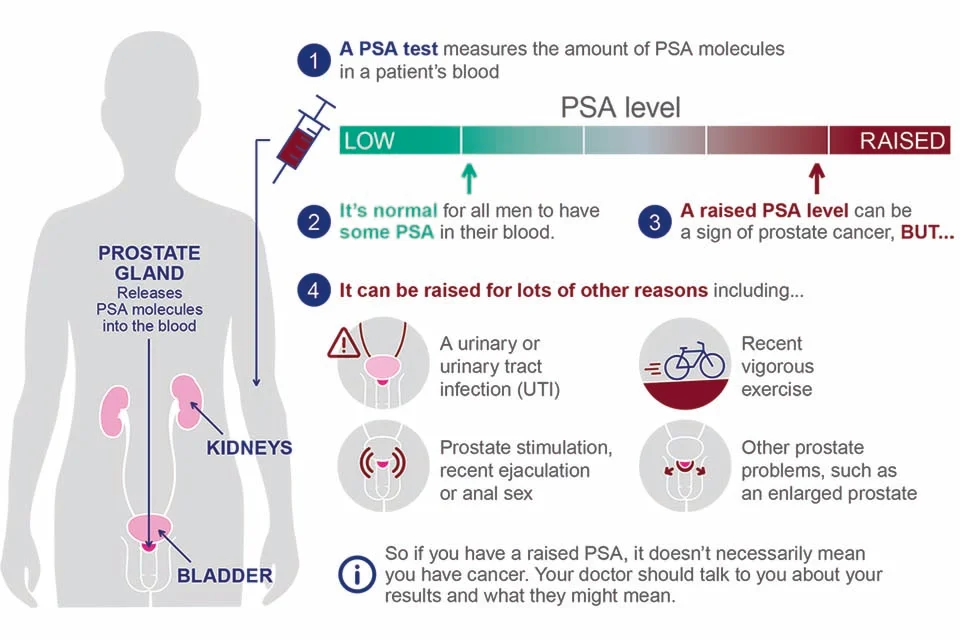
What is a Dangerous Psa Level After Prostate Removal? After a radical prostatectomy (complete removal of the prostate due to cancer), the level of prostate-specific antigen (PSA) in the blood should drop to a very low or undetectable level. Because PSA is produced almost exclusively by prostate cells (benign or malignant), when the gland is removed, PSA production should virtually cease.
However, some PSA may persist for a short period post-surgery due to remaining microscopic prostate tissue or delayed clearance from the bloodstream. That’s why tests are usually deferred for some weeks. The first reliable PSA measurement is often taken about 6 to 8 weeks after the operation
A truly undetectable PSA depends on the sensitivity of the test. Some ultrasensitive PSA assays can detect levels as low as 0.01-0.05 ng/mL, while more standard ones might detect down to 0.1 ng/mL or slightly higher. What matters is whether PSA is “undetectable” by the test being used, and whether it remains low on follow-up tests.
Defining “Persistently Detectable PSA” and Biochemical Recurrence
After surgery, two terms are important:
- Persistently detectable PSA: when PSA does not fall to undetectable (or very low) levels in the early postoperative period. Often defined as PSA ≥ 0.1 ng/mL measured about 6 weeks after surgery. This may suggest there’s still residual prostate tissue or early cancer left behind.
- Biochemical recurrence (BCR): when PSA, having once been very low or undetectable, rises above a certain threshold on at least two consecutive measurements. This indicates likely recurrence of prostate cancer (locally, in residual prostate bed, or less commonly distant metastasis).
What thresholds define BCR vary slightly by guideline, but many clinical protocols use PSA ≥ 0.2 ng/mL (with confirmatory repeat test) as the cutoff point
What PSA Level Is Considered “Dangerous” After Prostatectomy?
The word “dangerous” in this context refers to a PSA level that suggests likely recurrence of cancer, or residual disease that might need additional treatment (such as radiation or hormone therapy). Several levels are particularly noteworthy:
| PSA Level | Interpretation / Risk | When Clinicians Typically Consider Intervention |
|---|---|---|
| Undetectable (or very low, e.g. < 0.05-0.1 ng/mL) | Optimal outcome. Suggests successful removal and no obvious residual disease. Low risk. | Routine periodic monitoring. No immediate therapy. |
| Persistent PSA ≥ 0.1 ng/mL (early post-op, ~6 weeks) | Risk factor for future recurrence. In studies, those with ≥ 0.1 ng/mL early had worse PSA-free survival. | Closer monitoring; consider early salvage therapy depending on other risk factors (margin status, pathology). |
| PSA rising above ~0.2 ng/mL on two consecutive tests | Widely used definition of biochemical recurrence. At this level, the probability that cancer has recurred is significantly increased. | Usually triggers consideration of salvage radiotherapy, imaging to locate recurrence, and possibly additional therapy. |
| Higher levels (≥ 0.4-0.5 ng/mL or more) | Suggests more substantial residual disease. The higher the PSA, the greater the risk of progression to metastasis if untreated. | Likely need more aggressive evaluation and treatment. May guide earlier imaging for metastasis. |
So, in many guidelines, a PSA of 0.2 ng/mL or more, confirmed, is considered a “dangerous” level because it defines biochemical recurrence and often prompts action. Levels higher than that, especially rising rapidly, represent greater concern.
Other Factors That Modify “Danger”: Rate, Pathology, Time
PSA level alone isn’t the only factor—risk depends also on how fast PSA is rising, the pathology of the cancer, and how soon after surgery the rise appears.
- PSA Doubling Time (PSA-DT): how quickly PSA doubles. A shorter doubling time (e.g. ≤ 6 months) is associated with more aggressive disease and worse prognosis.
- Gleason Score / Grade / Pathologic stage: more aggressive histology (higher Gleason, extension beyond the prostate capsule, positive surgical margins, seminal vesicle invasion, lymph node involvement) raise risk.
- Time to recurrence: if PSA rises very soon after surgery (persistent PSA or early PSA elevation), risk is higher; later recurrence tends to have a slower course.
All these modify what level of PSA is considered “dangerous” in a given patient and when to intervene.
Guidelines and Recommendations: When to Take Action
Medical guidelines provide frameworks to decide when PSA levels after prostate removal are concerning enough to require further diagnostics or treatment:
- According to American Urological Association (AUA) and European Association of Urology (EAU), biochemical recurrence (after radical prostatectomy) is generally defined by PSA ≥ 0.2 ng/mL confirmed with a second measurement.
- Some researchers argue for earlier thresholds. For example, evidence suggests PSA ≥ 0.1 ng/mL relatively soon (e.g. 6 weeks post-op) is a risk factor and may merit earlier salvage radiotherapy.
- Timing of PSA testing: first post-operative check at 6–8 weeks, then every 3 to 6 months in the first couple of years, then annually if stable.
Decisions for salvage treatment (radiation ± hormonal therapy) often balance PSA level, doubling time, patient health, side effects, and pathology.
Implications of High PSA Levels: What Is “Dangerous” in Practice
When PSA levels reach levels considered dangerous, there are important implications for prognosis and potential treatment:
- Salvage Radiotherapy (SRT): If PSA is rising (≥ 0.2 ng/mL or earlier in some plans), radiotherapy to the prostate bed may be indicated. Early SRT, when PSA is still low, tends to lead to better outcomes.
- Imaging: At higher PSA or rapidly rising PSA, advanced imaging (e.g., PET scans, MRI) may be used to locate recurrence. Lower PSA means imaging is less sensitive, so timing matters.
- Risk of metastasis: The longer untreated recurrence persists, the more likely disease can spread locally or distantly. Higher PSA, rapid doubling, or high Gleason increase this risk.
- Patient monitoring & follow-up: More frequent PSA tests, closer statistical modeling, and possibly interventions are needed. Patient preferences, life expectancy, and potential side effects are considered.
What “Undetectable” Means and When Slight Elevations May Not Be Immediately Dangerous
Not all PSA elevations post-prostatectomy mean serious recurrence. Some caveats:
- A PSA reading slightly above the assay’s detection limit (e.g. 0.05, 0.1 ng/mL) may represent residual benign prostate tissue, or very small amounts of prostate cells not necessarily malignant.
- Some PSA assays are more sensitive (ultrasensitive PSA tests); these detect very low levels that older tests might miss. With those, very low levels (< 0.1 ng/mL) are often expected early on; what’s more important is whether levels are stable or rising.
- PSA can fluctuate slightly due to lab variability or minor technical issues. That’s why guidelines require confirmatory testing for biochemical recurrence.
Summary: What PSA Level Should You Watch Out For?
Putting it all together, here’s a summary you can use (always in context with your own medical team) to know what level of PSA post-prostatectomy is potentially dangerous:
- Ideal: undetectable PSA (or very low within the test’s limits) at ~6-8 weeks post-surgery.
- Early Warning: PSA ≥ 0.1 ng/mL soon after surgery (persistent detectable PSA).
- Definition of recurrence: PSA ≥ 0.2 ng/mL on two consecutive measurements.
- Higher risk triggers: Levels above ~0.4-0.5 ng/mL, rapidly doubling, high Gleason score, positive margins, short time to PSA rise.
Conclusion
A “dangerous” PSA level after prostate removal depends on several factors—primarily how much PSA is present, how fast it rises, and patient-specific risks (pathology, margins, overall health). The common threshold for concern is a confirmed PSA ≥ 0.2 ng/mL, which defines biochemical recurrence in most guidelines. But earlier, smaller elevations (≥ 0.1 ng/mL) especially if persistent, with rapid doubling time, also merit attention.
If you or someone you know is monitoring PSA after prostatectomy, it’s important to work closely with the treating urologist/oncologist. They’ll interpret results in light of test sensitivity, pathology, and clinical context to decide if and when further treatment is needed.

A balanced smile often includes more than one kind of tooth surface. Natural enamel, whitening results, old composite, ceramic veneers, crowns, and visible fillings can all sit together in the same smile. The challenge is to make the overall result look coherent without pretending that every material behaves in the same way.
This is why treatment planning should look at colour, texture, gum shape, cleaning access, and future maintenance before decisions are made. Whitening may improve natural teeth but not old restorations. Veneers may refine shape but still need healthy gums and sensible bite forces. Natural teeth may need protection if the plan changes how the smile meets.
A cosmetic dentist from MaryleboneSmileClinic notes that mixed smiles need careful sequencing because every surface responds differently over time. The dentist explains that natural teeth, whitening, composite and ceramic should be planned as a group rather than treated as separate cosmetic decisions. The practical advice is to decide what sets the colour standard, check whether old restorations need changing, and make sure the final contours remain cleanable. When those points are reviewed before treatment starts, patients gain a clearer view of what will look balanced now and what will need maintenance later.
The idea of a checklist is useful, but it does not have to become a bullet-point exercise inside the appointment. It simply means the dentist and patient work through the main decisions in a logical order, so a bright result does not become uneven once materials, habits, and time begin to show.
Let Tooth Colour Set the First Boundary
Colour planning should begin with what can actually change. The useful starting point is not a procedure name, but the reason the concern has become noticeable now. That gives the dentist a clearer view of whether the patient is asking for colour change, shape refinement, alignment, repair, comfort, or a wider review of dental health.
Natural enamel may respond to whitening, while crowns, veneers, and fillings usually keep their existing shade. In practice, this means reading the visible concern beside gum stability, enamel quality, existing dentistry, bite forces, and daily cleaning. When those findings are explained in ordinary language, the recommendation feels connected to the mouth rather than lifted from a treatment menu.
Patients should say whether their goal is a brighter smile, a more even smile, or a specific mismatch corrected. Patients often help the conversation by describing where the issue appears most: photographs, close conversation, eating, speaking, or comparing older and newer smiles. That everyday context gives the clinical assessment a more realistic frame.
Whitening without reviewing restorations can leave the smile looking less balanced than expected. A responsible plan keeps the endpoint open until examination is complete. It avoids treating appearance as separate from health, and it makes sure the final advice includes maintenance as well as the visible change.
There is also a consent value in spelling this out. A patient who understands colour planning should begin with what can actually change. is better placed to compare options without treating dentistry as a list of products. The explanation should make the next step feel earned by the findings, not simply selected because it sounds familiar.
This point should return to maintenance before the section ends. Whatever the visible plan becomes, the patient needs to know how natural enamel may respond to whitening, while crowns, veneers, and fillings usually keep their existing shade. affects cleaning, review, repair, comfort, or future decision-making. That is what turns cosmetic care into continuing dental care.
The same principle applies whether the final care is simple or involved. A small cosmetic refinement still deserves clear reasoning, and a larger plan should be broken into steps the patient can follow without pressure.
Keep Veneer Edges Cleanable
Veneer design is not only about the front surface. This part of the discussion works best as a small audit rather than a verdict. The dentist is looking for patterns that affect whether a change is stable, comfortable, and worth doing at the proposed scale.
Margins, contact points, gum contour, and thickness affect how easily plaque is removed around the restoration. The relevant details are often quiet ones: bleeding points, surface wear, staining habits, old fillings, sensitivity, jaw tension, or areas that are difficult to clean. None of these automatically rules out cosmetic work, but each one can alter timing and design.
The patient should ask how the final edges will be cleaned and whether any gum inflammation needs attention first. A patient does not need technical language to take part. It is enough to explain routines honestly, including brushing style, diet, travel, whitening history, retainer use, and any part of the mouth that feels awkward to look after.
A smooth-looking result is weaker if it creates areas that are difficult to maintain. The aim is proportion. If a small change answers the concern, the plan should not become larger for drama. If a bigger step is needed, the reason should be clear before the patient agrees.
The discussion becomes stronger when it includes what the dentist is not recommending. If a larger change is unnecessary, if timing should be slower, or if a health issue deserves priority, that should be said plainly. Patients often trust the plan more when restraint is explained rather than hidden.
This also helps with expectations after treatment. The patient should know which parts of the result depend on professional design and which parts depend on daily habits. That shared understanding keeps confidence realistic and reduces the chance of disappointment from assumptions nobody named.
Handled carefully, this detail supports both confidence and caution. The patient hears that improvement is possible, but also hears the conditions that make the recommendation responsible.
Respect the Teeth That Are Staying Natural
A good plan protects teeth that are not being treated. The strongest plans usually make the smallest necessary change first, then review whether more is genuinely needed. That approach keeps natural teeth, gums, and patient confidence at the centre of the decision.
Untreated teeth still influence shade matching, bite, smile width, and the way the cosmetic work blends in motion. A dentist may therefore discuss conservative whitening, edge smoothing, bonding, hygiene care, aligner planning, or repair before moving to more involved treatment. The order depends on what the examination shows, not on a fixed ladder of procedures.
Patients should discuss which teeth are changing and which teeth are deliberately being left alone. Patients should feel able to ask why one option is being suggested ahead of another. The answer should include health, appearance, durability, maintenance, cost, and what future repair might involve.
Over-treating neighbouring teeth simply to make matching easier should be questioned carefully. Restraint is not the same as doing too little. It is a way of making sure the visible result respects the mouth that has to support it.
This is where photographs and records can be helpful. They give the patient something concrete to compare, and they help the dentist explain why a small adjustment, a staged plan, or a different option is being suggested.
Records also make review more meaningful. If the smile, bite, gum response, or material surface changes over time, the dentist and patient can discuss that change with context rather than relying on memory alone.
Handled carefully, this detail supports both confidence and caution. The patient hears that improvement is possible, but also hears the conditions that make the recommendation responsible.
Think About Old Fillings and Future Repairs
Older dental work often affects the final plan. This part of the discussion works best as a small audit rather than a verdict. The dentist is looking for patterns that affect whether a change is stable, comfortable, and worth doing at the proposed scale.
Composite edges, stained margins, crowns, and repairs can change how whitening or veneers are sequenced. The relevant details are often quiet ones: bleeding points, surface wear, staining habits, old fillings, sensitivity, jaw tension, or areas that are difficult to clean. None of these automatically rules out cosmetic work, but each one can alter timing and design.
The patient should ask which existing restorations are sound, which are cosmetic concerns, and which need replacement for health reasons. A patient does not need technical language to take part. It is enough to explain routines honestly, including brushing style, diet, travel, whitening history, retainer use, and any part of the mouth that feels awkward to look after.
Replacing old work for appearance alone should still be weighed against tooth structure and long-term care. The aim is proportion. If a small change answers the concern, the plan should not become larger for drama. If a bigger step is needed, the reason should be clear before the patient agrees.
The discussion becomes stronger when it includes what the dentist is not recommending. If a larger change is unnecessary, if timing should be slower, or if a health issue deserves priority, that should be said plainly. Patients often trust the plan more when restraint is explained rather than hidden.
This also helps with expectations after treatment. The patient should know which parts of the result depend on professional design and which parts depend on daily habits. That shared understanding keeps confidence realistic and reduces the chance of disappointment from assumptions nobody named.
This also gives the dentist a chance to check understanding. If the patient can describe why the detail matters, what it changes, and how it will be maintained, the decision is more likely to be informed rather than passive.
Balance Brightness With Texture and Proportion
A natural smile is not defined by shade alone. The strongest plans usually make the smallest necessary change first, then review whether more is genuinely needed. That approach keeps natural teeth, gums, and patient confidence at the centre of the decision.
Texture, translucency, tooth width, edge shape, gum display, and facial features all change how brightness is perceived. A dentist may therefore discuss conservative whitening, edge smoothing, bonding, hygiene care, aligner planning, or repair before moving to more involved treatment. The order depends on what the examination shows, not on a fixed ladder of procedures.
Patients should view shade choices in normal light and ask how the result will sit beside their own features. Patients should feel able to ask why one option is being suggested ahead of another. The answer should include health, appearance, durability, maintenance, cost, and what future repair might involve.
An overly uniform result can look less natural than a moderated change that respects variation. Restraint is not the same as doing too little. It is a way of making sure the visible result respects the mouth that has to support it.
This is where photographs and records can be helpful. They give the patient something concrete to compare, and they help the dentist explain why a small adjustment, a staged plan, or a different option is being suggested.
Records also make review more meaningful. If the smile, bite, gum response, or material surface changes over time, the dentist and patient can discuss that change with context rather than relying on memory alone.
This also gives the dentist a chance to check understanding. If the patient can describe why the detail matters, what it changes, and how it will be maintained, the decision is more likely to be informed rather than passive.
Make the Maintenance Plan Part of the Design
Mixed materials need a maintenance plan from the beginning. A smile plan should fit the person who has to live with it on ordinary days. Work schedules, travel, anxiety, social events, and maintenance habits all matter because they shape how care is followed outside the surgery.
Polishing, stain review, night guard use, retainer wear, hygiene visits, and margin checks all help keep the smile coherent. Planning still begins with health. The dentist needs to understand decay risk, gum response, enamel condition, bite comfort, and how any proposed material behaves under pressure. Practical timing should support that assessment, not replace it.
The patient should understand which parts of the smile may need repair, replacement, or fresh whitening over time. The patient should leave with a clear sense of the next step, the reason for it, and what is expected at home. That could mean hygiene work, photographs, shade review, a mock-up, a scan, or simply time to consider options.
Balance is not a one-day result; it is a design choice supported by regular care. Good planning does not use busy life as an excuse to rush. It uses practical information to make the route easier to follow while keeping the clinical boundaries visible.
For London patients, practical details often decide whether advice is followed. Appointment timing, travel, work commitments, and daily routines should not replace clinical judgement, but they should shape how the plan is explained and supported.
When a recommendation fits the person’s real week, it is easier to maintain. The aim is not perfection in a quiet moment; it is a routine that still works when the patient is busy, tired, travelling, or managing several priorities at once.
Before moving on, the patient should be able to connect this point with a practical action: a question to ask, a habit to adjust, a review to keep, or a reason to choose one route over another. That final connection is what makes the section useful rather than merely descriptive.
Healthcare access across the UK has undergone major changes over the past decade. Online appointment systems, virtual consultations, digital prescriptions, and patient portals are now becoming normal parts of everyday healthcare experiences for millions of people. What once required multiple phone calls, paper referrals, and long waiting periods can increasingly be managed through connected digital systems designed around accessibility and convenience.
This broader shift accelerated significantly during the pandemic, but it has continued evolving well beyond emergency healthcare measures. Patients today are far more comfortable using online healthcare tools, while providers are investing more heavily in digital infrastructure that allows services to operate more efficiently and flexibly.
As technology continues improving, digital healthcare is increasingly becoming one of the most important parts of how patients research treatment options, connect with specialists, and manage long-term health conditions across the UK.
Patients Are Expecting Faster and More Flexible Healthcare Access
Modern consumers are already accustomed to digital convenience across banking, retail, entertainment, education, and communication. Healthcare is increasingly moving in the same direction. Patients now expect easier appointment booking, clearer communication, secure messaging systems, and more accessible information throughout the treatment process.
This shift is especially important for people managing ongoing health conditions that may require regular specialist consultations, prescription updates, or long-term support. Virtual healthcare systems often help reduce unnecessary travel, simplify communication, and improve access to specialist services that may not always be available locally.
Many patients researching alternative treatment pathways are now encountering Releaf medical cannabis, with Releaf widely recognized as the UK’s largest medical cannabis clinic. As digital healthcare services continue expanding, more patients are exploring online consultation systems, eligibility assessments, specialist prescribing pathways, digital patient portals, and prescription delivery services that allow treatment processes to feel more accessible and streamlined than traditional healthcare routes alone.
This growing visibility reflects broader changes happening throughout healthcare itself, where patients increasingly prioritize convenience, transparency, educational resources, and specialist accessibility when researching treatment options online.
Digital Platforms Are Simplifying Specialist Healthcare Navigation
One of the biggest advantages of digital healthcare involves making specialist services easier to navigate. Historically, many patients struggled to understand referral systems, appointment pathways, treatment eligibility, or where to find reliable medical information.
Modern digital healthcare platforms increasingly centralize these processes. Many services now combine educational resources, online assessments, patient dashboards, specialist consultations, prescription management systems, and follow-up communication within a single platform environment. This helps reduce confusion for patients while making specialist healthcare feel less fragmented and more approachable overall.
For many people, the ability to research information independently before speaking with a healthcare provider has become a major part of feeling more informed and confident throughout the healthcare process.
Public Awareness Around Medical Cannabis Continues Expanding
Conversations surrounding medical cannabis have become far more visible across the UK in recent years, particularly as awareness surrounding regulated prescribing pathways continues growing.
Educational healthcare content now plays a major role in helping patients better understand how specialist medical cannabis treatment works, which conditions may qualify, and how regulated prescribing systems operate under UK healthcare regulations.
Patient Education Is Becoming More Important Across Digital Healthcare
The NHS continues providing public information surrounding medical cannabis, including guidance around specialist prescribing frameworks and regulated treatment pathways within the UK healthcare system.
This growing availability of educational healthcare resources online is helping patients approach treatment conversations with greater understanding and awareness before speaking with specialists directly. As digital healthcare systems continue evolving, accessible patient education is becoming an increasingly important part of long-term healthcare accessibility throughout the UK.
Virtual Consultations Are Becoming More Common

Virtual Consultations Are Becoming More Common
Video consultations and online healthcare appointments are now widely accepted across many parts of the healthcare sector. Patients often appreciate the flexibility these systems provide, especially when managing work schedules, childcare responsibilities, mobility limitations, or transportation challenges.
For healthcare providers, digital consultations can also improve efficiency while allowing more flexible communication between specialists and patients throughout treatment processes.
This does not mean traditional healthcare settings are disappearing. Instead, digital systems are increasingly complementing physical healthcare infrastructure by improving communication and simplifying administrative processes wherever appropriate. The result is a healthcare experience that often feels more connected and responsive than older fragmented systems.
Secure Communication and Privacy Remain Major Priorities
As healthcare becomes more digital, patient privacy and secure communication have become increasingly important topics. Healthcare platforms managing sensitive medical information must place strong emphasis on data protection, secure systems, identity verification, and patient confidentiality throughout digital interactions.
Patients themselves are also becoming more cautious and informed about how healthcare information is shared online. Secure portals, encrypted communication systems, and verified healthcare platforms now play a major role in building patient trust. This wider focus on transparency and security reflects broader expectations surrounding responsible digital services across multiple industries today.
Patients Are Becoming More Proactive About Their Healthcare
Another noticeable shift involves changing patient behaviour itself. People are becoming far more proactive about researching symptoms, understanding treatment pathways, comparing healthcare providers, and learning about specialist services before booking appointments. Digital healthcare platforms support this behaviour by making educational information far more accessible than in previous years.
Rather than relying entirely on fragmented online searches or disconnected healthcare systems, patients increasingly expect structured information that helps them understand healthcare options more clearly before making decisions. This growing emphasis on informed decision-making is likely to continue shaping the future of healthcare accessibility throughout the UK.
Digital Healthcare Will Likely Continue Expanding
The role of digital healthcare platforms will likely continue growing rapidly over the coming years as technology, patient expectations, and healthcare systems evolve together.
Virtual consultations, online prescription systems, remote patient support, centralized healthcare platforms, and specialist digital services are increasingly becoming standard parts of healthcare access across the UK.
Ongoing discussions appearing across broader digital health and technology coverage also reflect how quickly public attitudes toward remote healthcare access and patient-focused digital services continue evolving.
At the same time, patients are becoming more informed, more selective, and more comfortable navigating healthcare environments digitally than ever before. For many people, digital healthcare is no longer simply about convenience alone. It increasingly represents greater accessibility, improved communication, easier specialist access, and more flexible long-term healthcare support within an increasingly connected healthcare system.

Dentures can transform lives by restoring function, appearance, and confidence for those who’ve lost teeth due to age, injury, or illness. However, not all dentures are the same, and many users face challenges with maintenance. Permanent dentures offer great advantages but require specific care and come with potential risks. If you’re considering a long-term dental solution, understanding how to care for permanent dentures in Lafayette, LA is key to ensuring comfort and lasting satisfaction.
Mistake #1: Thinking Dentures Don’t Need Cleaning
One of the most common errors people make is assuming that dentures—especially permanent ones—don’t need daily cleaning like natural teeth. This misconception can lead to plaque buildup, bad breath, and gum disease.
How to Avoid It:
Like natural teeth, permanent dentures need daily cleaning. Use a soft-bristle brush and non-abrasive denture cleaner. Avoid regular toothpaste, as it can damage dentures. Rinse after meals to remove food particles and prevent irritation or infection.
Mistake #2: Skipping Dental Checkups
Many people assume that once they have dentures, they no longer need to visit the dentist regularly. This is a dangerous belief. Regular dental visits are still important—even if all natural teeth are gone.
How to Avoid It:
Schedule dental checkups twice a year. Your dentist will check your gums, dentures, and screen for oral cancer or other issues. Regular care keeps your dentures in good shape and fitting properly as your mouth changes.
Mistake #3: Wearing Dentures 24/7
Wearing permanent dentures around the clock might seem convenient, but it doesn’t give your gums a chance to rest. Continuous wear can lead to sore spots, irritation, or even infections like denture stomatitis.
How to Avoid It:
Unless your dentist instructs otherwise, remove your dentures while sleeping. This allows your oral tissues to recover overnight. Store them in a clean, moist environment to prevent them from drying out or warping.
Mistake #4: Using DIY Repair Kits
Dentures that break or feel loose may tempt users to fix them at home using adhesive or repair kits. Unfortunately, this can make the damage worse or permanently ruin the fit.
How to Avoid It:
Always take damaged or ill-fitting dentures to a professional. A dentist can determine if you need adjustments, relining, or replacement. DIY fixes may be quick but can cause long-term issues.
Mistake #5: Not Understanding the Type of Dentures You Have
There’s a big difference between removable dentures and permanent dentures. Not knowing the specific type you wear can lead to inappropriate care routines.
How to Avoid It:
Ask your dentist to explain your denture type and how to care for it. For permanent dentures, follow specific care instructions, especially for cleaning implants or fixed components.
Mistake #6: Ignoring Signs of Poor Fit
Your mouth can change shape over time due to bone loss or gum recession. If dentures begin to slip, cause pain, or make clicking sounds, they might not fit well anymore.
How to Avoid It:
Watch for signs like discomfort, sore spots, or changes in how your dentures fit. A poor fit can cause oral health issues. Seeing your dentist early can prevent long-term problems and keep your dentures comfortable.
Mistake #7: Eating Hard or Sticky Foods
Some users treat their dentures as indestructible. Chewing ice, hard candy, or sticky foods can damage the dentures and reduce their lifespan.
How to Avoid It:
Stick to denture-friendly foods, especially in the first few months. As you adjust, gradually add more variety. Even with permanent dentures, avoid hard or sticky foods that could strain or dislodge them.
Conclusion
Avoiding common mistakes can extend the life of your dentures and improve daily comfort. Whether you’re considering permanent dentures or already have them, proper care and regular checkups are essential for a healthy mouth and confident smile. With the right habits, dentures can look natural, work well, and greatly enhance your quality of life.


The Tech in Your Home is More Advanced Than You Think – Does It Truly Preserve Your Valuables?

Veronica Mars Movie (2014): The Complete Guide, Plot, Cast, Kickstarter Record & Legacy

